 The Independent Uganda: You get the Truth we Pay the Price
The Independent Uganda: You get the Truth we Pay the Price


On June 12, the Ministry of Health, WHO, Center for Disease Control (CDC), the Resident District Commissioner (RDC) – Kasese and the Ministry of Health, DRC led by Gaston Tshapenda held a joint meeting to discuss the issue.
They resolved that all the unofficial points of entry would be manned on both Ugandan and DRC sides and information on any unusual event shared immediately.
At the same meeting, DRC proposed the repatriation of the five Ebola patients, including the mother of the deceased 5 year old, his two brothers, father and their domestic worker. These were successfully repatriated on June 13.
Uganda health minister says that these were repatriated in order for them to access medicines for therapeutic treatment which are available in the DRC as well receive family support.
Uganda’s reaction is informed by the many times the Ebola virus and other deadly hemorrhagic fevers have struck the country. Outbreaks in 2000, 2012 and 2017 have prompted the health ministry to build capacity.
At the end of May, the government of Uganda and other key stakeholders invested over US$18 million in Ebola virus preparedness and readiness at an Accountability Forum.
The government of Ireland through the Irish embassy also contributed US$1million towards the preparedness for Ebola.
“As an embassy that has spent 25 years in Uganda, we wanted to provide logistical support and strengthen health and make sure the medicines are made available to each and every individual. That is why we stepped in”, said Aine Doody the head of cooperation at the embassy of Ireland.
In a precautionary move, the health ministry has vaccinated some 4,700 health workers in more than 150 facilities with an experimental drug designed to protect them against the virus, which spreads through contact with bodily fluids of those infected, causing hemorrhagic fever with severe vomiting, diarrhea and bleeding.
The vaccine is experimental but is estimated to be 97.5% effective and, according to the WHO, may protect a person for up to 12 months.
The WHO has offered 30 motorcycles and two multipurpose vehicles to help in surveillance. The Ministry of health is ensuring that non-gazetted places at borders do thorough screening.
“We have received 400 doses from the Democratic Republic of Congo (DRC) and over 4000 doses from WHO which are going to be used in the ring vaccination of contacts and heath workers who were at the frontline unvaccinated,” Aceng said.
Rates of infection
According to the Ministry of Health, there were three suspected cases of Ebola and over 78 contacts. Of the suspected cases, two tested negative and only one is infected.
However, the ministry warns that the situation in DRC is scary and Uganda is still at a high risk of contracting the virus. It is estimated that there are over 2000 Ebola cases and over 1000 deaths of Ebola in the DRC.
“Each and every person should be alert. I want the entire nation to observe a no handshaking/body contact phase until we are Ebola free. I also want to appeal to you all to always wash your hands with soap or jik and water”, said Aceng.
Tariq Riebl, the Emergency Response Director of the International Rescue Committee in the DRC says although the Ebola outbreak in the DRC was not declared an international emergency, the spread of Ebola to Uganda is a clear signal that the international community must reset and redouble its efforts to work with the Congolese people and stop the spread of the disease here in the DRC.
“While Uganda is well prepared to handle this outbreak in the country, as long as the disease continues to spread in the DRC, we will continue to see cases cross international borders and into neighboring countries”.
Tackling the Ebola outbreak in DRC has been complicated by conflict in the region – between January and May there were more than 40 attacks on health facilities. Another problem is distrust of healthcare workers with about a third of deaths being in the community. It means people are not seeking treatment and risk spreading the disease to neighbours and relatives.
About Ebola
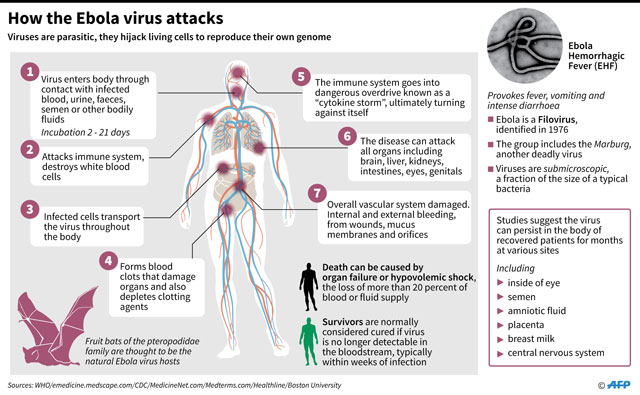
Ebola virus was first discovered in 1976 near the Ebola River in what is now the Democratic Republic of Congo. Since then, the virus has been infecting people from time to time, leading to outbreaks in several African countries. Scientists do not know where Ebola virus comes from.
However, based on the nature of similar viruses, they believe the virus is animal-borne, with bats being the most likely source. The bats carrying the virus can transmit it to other animals, like apes, monkeys, duikers and humans.
Ebola virus spreads to people through direct contact with bodily fluids of a person who is sick with or has died from it. This can occur when a person touches the infected body fluids (or objects that are contaminated with them), and the virus gets in through broken skin or mucus membranes in the eyes, nose, or mouth. The virus can also spread to people through direct contact with the blood, body fluids and tissues of infected fruit bats or primates. People can get the virus through sexual contact as well.
Ebola survivors may experience difficult side effects after their recovery, such as tiredness, muscle aches, eye and vision problems and stomach pain. Survivors may also experience stigma as they re-enter their communities.
The signs and symptoms include; fever, severe headache, muscle pain,weakness, fatigue, diarrhea, vomiting, abdominal (stomach) pain and unexplained hemorrhage(bleeding or bruising).
****



